

Inherited motor neurone disease (MND)
Glossary and explanation of key terms
Motor Neurone disease (MND)
MND is a neurodegenerative condition that affects the motor neurons, which are nerves that send signals from the brain to the muscles to make them move. MND is also known as motor neuron disease, amyotrophic lateral sclerosis (ALS) or Lou Gehrig’s disease. MND affects people differently but leads to weakness and wasting of muscles, which gets worse over time. This can cause loss of mobility in the limbs, and difficulties with speech, swallowing and eventually breathing. MND is sometimes categorised according to the initial symptoms (e.g. bulbar or lower-limb onset) or the pattern of progression. All of these categories still come under the term ALS, with the exception of a very rare group who have a type of MND known as primary lateral sclerosis (PLS) (more information about these can be found on the MND Association website). It is thought that most cases of MND are caused by a combination of genetic and environmental factors, and that there are multiple steps needed for a person to develop the disease, though scientists don’t fully understand what these are yet. In a minority of cases MND is caused by a single genetic variant (see below) that can be passed down in families. We call this inherited MND, but it is sometimes called familial MND or familial ALS. This section of the website focuses on inherited forms of MND.
Frontotemporal dementia (FTD)
Frontotemporal dementia is a type of dementia that may cause personality and behaviour changes, language problems, and difficulties with concentration, planning and organisation. Some families affected by MND also have a family history of frontotemporal dementia (FTD). This is because there are some genetic variants which can cause both conditions, as well as other neurological symptoms. People who have inherited these genetic variants may develop either MND or FTD, but some people develop both at the same time. A repeat expansion of the C9orf72 gene (see ‘gene repeat sequences’ below) is the most common genetic cause of MND and FTD in people from a white European background but is much rarer in Asian populations where other genes may be associated with an increased risk of MND and FTD instead.
Genes and gene variants
Genes are the instruction manuals which tell our body how to make proteins, which in turn make our bodies work and grow. We have two copies of every gene, one inherited from each parent. Genes are carried in a structure called DNA, which is itself organised into a bigger structure called a chromosome. Under a microscope, DNA looks like two strands which wind around each other in a double helix shape. Each strand is formed of building blocks which scientists call ‘bases’, represented by the letters A C G and T. Genes are sections of DNA, made up of particular sequences of these bases.
When our bodies make new cells, they have to ‘copy and paste’ our DNA. Sometimes there are errors made in this process, which can affect how the body works. At other times, changes are caused by external factors like smoking or radiation. When a change is present in the sperm or egg cells (germ cells), they can be inherited from a parent or changes can occur when the egg and the sperm come together to make the first cells of a baby.
Lots of the time, changes are harmless, and we all carry genetic changes that are just part of normal variation and make each individual unique. However, other changes can disrupt how a gene functions. In some cases, this can cause certain diseases to develop. For example, see ‘gene repeat sequences’ below. Changes in genes are sometimes called ‘mutations’. We use the term ‘gene variant’ to describe a gene change, though you might also see the term ‘pathogenic gene variant’ used. This means a gene change that can cause disease. The Genetic Alliance UK website has more information on DNA, genes and chromosomes.
C9orf72, SOD1, and other gene variants linked to inherited MND
Scientists have discovered many genes associated with MND. The most studied genes are linked to inherited MND and significantly increase a person’s risk of developing the disease. These include C9orf72, SOD1, FUS and TARDBP. In people from a white European background, C9orf72 gene variants account for approximately 40% of cases of inherited MND, SOD1 for 20% and FUS and TARDBP for less than 5% each. In continental Asian populations, a higher proportion of inherited MND is caused by SOD1 gene variants and a much lower proportion is caused by C9orf72 gene variants. Scientists are continually discovering new genes associated with inherited MND and genes with changes that might increase an individual’s risk of developing MND. Other ‘variants of unknown significance’ (VUSs) may occur in genes associated with MND, which may or may not cause disease. Research in the future may help scientists to better understand their significance.
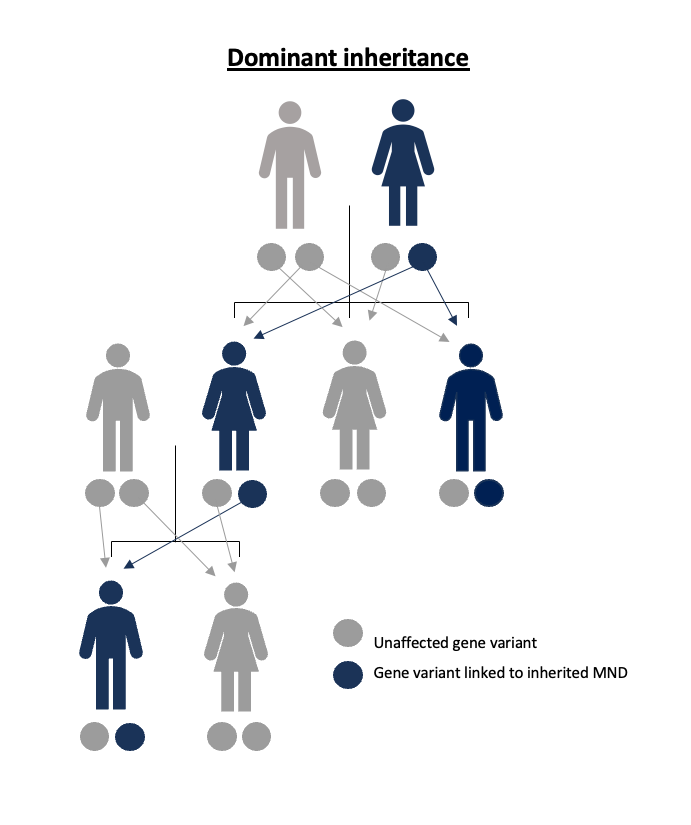
Inheritance
Inheritance refers to the way genetic characteristics are passed between parents and their children. We all carry two copies of each of the approximately 20,000 genes, one inherited from each parent. Most of the gene variants associated with inherited MND, including the most common variants mentioned above, are inherited in what is called a ‘dominant’ pattern. An affected parent would have one normal copy of the gene and one copy with a change that could increase the risk of MND (pathogenic gene variant). Only one parent needs to carry one copy of a dominant gene variant linked to inherited MND for it to be potentially passed on to their children. Each of their children has a 50% chance of inheriting the gene variant that increases the risk of MND, and a 50% chance of inheriting the normal copy of the gene. In each pregnancy the risk of this happening is the same; it isn’t affected by sex, number of siblings, or whether the child shares other characteristics with the affected parent. A person carrying a gene variant linked to inherited MND will not necessarily develop symptoms in their lifetime.
Penetrance
Penetrance refers to the proportion of people who carry a particular gene variant who will develop symptoms of the associated condition in their lifetime. Where a gene variant is described as having incomplete penetrance, not everyone who carries this gene variant will develop the disease. This depends on a combination of environmental and other genetic factors. It is not currently possible to define exactly what these are and what they mean in terms of an individual’s risk.
Gene repeat sequences
The normal structure of the C9orf72 gene consists of a sequence of six bases (see 'genes and gene variants' above) with the code ‘CCGGGG’, repeated over and over again. Many other genes also contain repeat sequences, and repeating sequences may have important roles in how genes work. The number of repeats that each individual has on each of their copies of the gene can be variable, but when a repeat sequence expands beyond a certain size, it can then be associated with an increased risk of developing a disease like MND. Scientists study unaffected individuals to understand the range of repeat sizes which are 'normal'. If a person has a higher than normal number of repeats, they are said to have a 'repeat expansion' which increases the chance of developing a certain disease, and they may pass this gene variant to their own children. In genes linked to inherited MND, like C9orf72, it is not completely understood how the number of repeats in the gene impacts a person’s chance of developing symptoms (including, for example, how the number of repeats could be linked to the age of onset). It is not always possible for a person to find out exactly how many repeats they carry. Sequences can be very long, and it is likely that the number of repeats can vary in different cells of the body, and might change over time.
De novo mutations
Most people who carry a gene variant associated with inherited MND will have inherited this from a parent, but these changes may also occur for the first time in an individual. This is called a 'de novo mutation' and happens by chance when the egg and the sperm come together to make the first cells of a developing baby. These changes may then be passed on to later generations and increase their risk of developing the condition.
Genetic counselling
People may choose to talk to a genetic counsellor for many reasons. Genetic counsellors can provide information on genetic conditions, helping people to understand how they and their relatives might be impacted, and offer support in adjusting to and coping with this knowledge. Genetic counsellors can share information on genetic testing and help people think through the implications of having a genetic test. They can also provide information on family planning options for people who have a genetic disorder in their family. Genetic counsellors aim to make sure people are well informed and can make the choices that are right for them. Some people who have been diagnosed with MND may benefit from genetic counselling before genetic testing, and in the UK, Genetic counselling is recommended before having a pre-symptomatic genetic test. A referral to a genetic counsellor does not mean that a test has to be carried out, and some people might go to a genetic counsellor to talk about genetic testing but decide not to be tested at that time. Genetic counsellors can also signpost to relevant resources, and sometimes refer people to other services too, such as psychological support. People who would like to talk to a genetic counsellor should go to their GP, who can make a referral. Some people might also benefit from talking to a neurologist.
Genetic testing after a diagnosis of MND
Genetic testing may be offered to people diagnosed with MND, particularly when it is clear that other family members have been affected by MND or FTD. It involves a blood test to look at the structure of a person’s genes, with the aim of finding out if the condition is caused by a change in any of the genes known to be linked to inherited MND. Genetic testing cannot be used in isolation to make a diagnosis of MND. A diagnosis of MND can only be made based on a person’s symptoms, by an experienced neurologist.
Pre-symptomatic genetic testing
Pre-symptomatic genetic testing (sometimes called predictive testing) is available to some people who do not currently have symptoms of MND but have a family history of MND or FTD. Pre-symptomatic genetic testing is only possible where a particular genetic variant associated with inherited MND has already been identified in an affected family member. It involves a blood test, which allows people without symptoms to find out if they have inherited the particular gene variant found in their family member. If the individual is found to carry the gene variant (a positive result), this means they have an increased risk of developing symptoms of MND, but the exact chance of this happening is sometimes hard to predict depending on the gene involved, as not everyone who carries a gene variant will develop the disease in their lifetime (see ‘penetrance’). Deciding whether to have pre-symptomatic genetic testing is an individual choice, with many factors involved in making the decision.
Pre-implantation genetic testing (PGT)
PGT uses the fertility treatment IVF (in vitro fertilisation) with the added step of genetic testing, and is available to some people who are at risk of passing on an inherited condition to their children. Embryos are produced through IVF and tested for the gene variant at a very early stage. Only embryos which do not carry the genetic variant would be transferred to the womb. This is sometimes also called PGD, preimplantation genetic diagnosis.
Pre-natal testing for inherited MND
Pre-natal testing for inherited MND involves testing an established pregnancy for the genetic variant (pre-natal means ‘before birth’). This type of testing is sometimes called PND or pre-natal diagnosis. Pre-natal testing can be carried out as early as 11+ weeks of pregnancy using Chorionic Villus Sampling (CVS) to collect a sample of DNA from the pregnancy. Having a prenatal test is associated with an increased risk of miscarriage, and people wouldn’t be advised to choose this option if they would not consider terminating the pregnancy if the fetus was found to carry the genetic variant. Testing a pregnancy but not having a termination after a positive test result would take away the child’s right to choose whether to have the genetic test later in life (The MND Association provide information on options when starting a family for people affected by inherited MND).
Randomised controlled clinical trials
The aim of randomised controlled clinical trials is to assess the safety and effectiveness of drugs or treatments, including new treatments. They aim to understand if drugs or treatments work better than current treatments, or nothing at all. Participants in these studies are put into different treatment groups, allocated by chance, and their results compared. One of the groups may get allocated to a placebo group and receive an inactive or ‘dummy’ treatment. In this way, researchers can be certain that any effects are due to the active drug. Participants do not know whether they are taking the active medicine or not until the end of the study. Some people may choose not to know which group they were in.
Cohort ‘observational’ studies
Cohort studies involve observing a group of individuals over a period of time. This sort of research may not directly or immediately benefit the participants but is designed to understand more about MND and find new ways to monitor disease activity and test future treatments. Participants in such studies may be asked to answer questions about themselves, give samples such as blood or spinal fluid, have specialised brain scans, and perform tests. Some studies may involve taking part just once and others may involve having tests at particular intervals over a period of time (for example, once a year). Depending on the design of the study, test results may or may not be shared with participants.
Gene therapies
Gene therapies refer to any medicines that target specific disease-causing genes, aiming to either block or enhance their effects. Gene silencing or protein lowering are techniques that could target specific genes associated with inherited MND.
Copyright © 2024 University of Oxford. All rights reserved.